Founder
Full Support
Managed Routinely
Training
Antegrade Dissection Re-entry (ADR) is one of the three crossing strategies in the Hybrid CTO Algorithm – the international consensus framework for chronic total occlusion intervention. When direct wire navigation through a CTO is not possible – typically because of an ambiguous or heavily calcified proximal cap, a long or tortuous occlusion, or failed antegrade wiring – ADR provides an alternative forward approach.
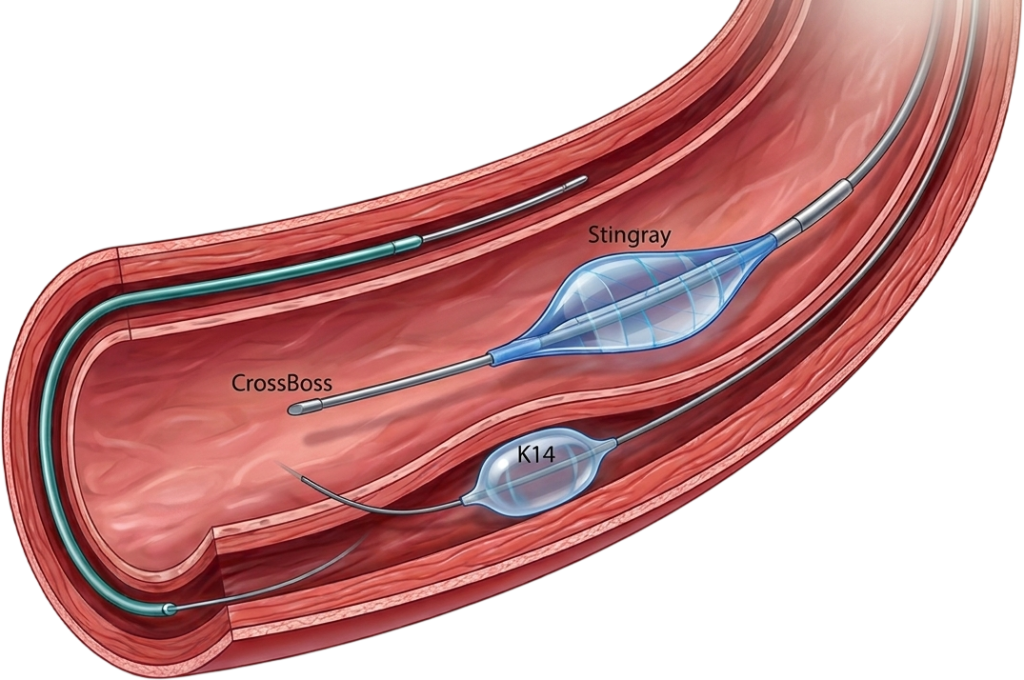
The technique uses two dedicated devices manufactured by Boston Scientific. The CrossBoss catheter is a blunt-tipped microcatheter that creates a controlled dissection in the subintimal space running alongside the CTO body. The Stingray balloon system – a flat, self-orientating, over-the-wire balloon with two opposing exit ports – is then inflated in the subintimal space beyond the blockage. A dedicated Stingray puncture wire is steered through one of the exit ports back into the true lumen of the vessel distal to the occlusion, allowing stenting from the re-entry point back to the proximal cap.
ADR accounts for 20–34% of CTO PCI cases in major hybrid operators’ registries internationally, and is considered a pillar of the hybrid algorithm for treating long, complex CTOs where wire-based approaches alone are unlikely to succeed.
The Hybrid CTO Algorithm specifies clear anatomical and procedural triggers for choosing ADR over wire-based antegrade approaches. The decision is made before resorting to prolonged failed wiring – which wastes radiation dose, contrast volume, and procedural time without changing the anatomy.
A polymer-jacketed wire is advanced into the subintimal space proximal to the CTO and knuckled (looped) to create a blunt leading edge. The knuckle is advanced through the subintimal space alongside the occlusion. Alternatively, the CrossBoss catheter is used with rapid rotational advancement to create a controlled subintimal channel - particularly useful in in-stent CTOs.
Once the subintimal channel has been extended past the distal cap of the CTO, the Stingray balloon is advanced over a wire into position. The balloon is flat with two opposing exit ports. After flushing with contrast, the balloon is inflated to 4 atmospheres in the subintimal space, where it self-orientates flat against the vessel wall and presents one port facing the true lumen.
Under fluoroscopic guidance in two orthogonal views, the Stingray puncture wire (or a stiff penetration wire such as Conquest Pro) is advanced through the exit port pointing toward the true lumen. Contralateral angiography confirms the wire has entered the true lumen and not deeper subintimal space. The "monorail sign" of the inflated Stingray balloon confirms correct orientation before puncture.
Once true lumen entry is confirmed in at least two angiographic projections, the Stingray balloon is deflated and removed. A workhorse wire is exchanged in, the microcatheter is advanced to the distal vessel, and the CTO segment is predilated. imaging-guided drug-eluting stent placement from the proximal landing zone through the subintimal channel to the distal true lumen completes the procedure.
The K14 technique addresses a specific and previously unsolved failure mode in standard Stingray re-entry: when the Stingray wire does not adequately penetrate through the Stingray port into the true lumen.
This happens most often when the subintimal space adjacent to the Stingray port is too narrow or fibrotic to accommodate the wire trajectory, or when the wire repeatedly deflects rather than punching cleanly through into the lumen. Until 2023, the recourse was to escalate to retrograde technique – a longer, more complex approach with higher complication risk.
Dr. Arun’s modification uses a CART (Controlled Antegrade and Retrograde Tracking) manoeuvre within the antegrade system to overcome this resistance. A small balloon is advanced into the subintimal space adjacent to the Stingray port and inflated – enlarging the space between the subintimal channel and the true lumen. The Stingray wire can then be steered accurately across the now-enlarged gap into the true lumen.
K14 stands for Kalyanasundaram – Dr. Arun’s nickname from his fellowship days at the Cleveland Clinic. The technique was published in Catheterization and Cardiovascular Interventions in 2023, with two case examples demonstrating successful re-entry after conventional ADR and Reverse-CART had failed. It has been adopted internationally and is taught at major CTO PCI courses across the Asia-Pacific.
Stingray CART (K14 technique): A novel antegrade dissection reentry strategy
Catheterization and Cardiovascular Interventions
2023
36617386
Arun Kalyanasundaram, MD
Ravi S. Hira, MD · William L. Lombardi, MD
Adopted internationally; referenced in Asia-Pacific CTO Club teaching materials
Standard ADR Fails
Stingray balloon is positioned and inflated. The Stingray puncture wire is advanced through the port toward the true lumen but cannot achieve clean re-entry – deflecting, buckling, or entering deeper subintimal tissue.
CART Balloon Inflation Adjacent to Stingray
Re-positioning and Re-puncture
Wire Exchange and Completion
Workhorse wire exchange, microcatheter advancement to the distal vessel, predilation, and imaging-guided drug-eluting stent placement from proximal landing zone through subintimal channel to distal true lumen.
CTO PCI — All Three Crossing Strategies
Retrograde CTO PCI
About Dr. Arun Kalyanasundaram
K14 Stingray CART is a novel antegrade dissection re-entry strategy invented and published by Dr. Arun Kalyanasundaram in Catheterization and Cardiovascular Interventions in 2023, PMID 36617386. It addresses a specific failure mode in standard Stingray re-entry where the wire cannot adequately penetrate from the subintimal space into the true lumen. The technique uses a CART manoeuvre to enlarge the adjacent space, allowing accurate wire passage. K14 stands for Kalyanasundaram - Dr. Arun's nickname from fellowship days at the Cleveland Clinic.
Antegrade Dissection Re-entry is one of the three crossing strategies in the Hybrid CTO Algorithm. It is used when direct antegrade wire navigation through the occlusion is not possible - typically because of an ambiguous or heavily calcified proximal cap, a long or tortuous occlusion, or failed antegrade wiring. The CrossBoss catheter creates a controlled subintimal dissection alongside the CTO. The Stingray balloon system then re-enters the true lumen of the vessel beyond the blockage. ADR accounts for 20–34% of CTO PCI cases in major hybrid operators' registries.
K14 is used as an advanced manoeuvre during antegrade dissection re-entry when standard Stingray re-entry has failed and the Stingray wire cannot achieve true lumen entry through the Stingray port. In the published cases, K14 was performed after conventional ADR and Reverse-CART approaches had been unsuccessful. It is an escalation technique within ADR - not a first-line approach.
The CrossBoss catheter is a blunt-tipped microcatheter that creates a controlled subintimal channel through a CTO when direct guidewire crossing fails. The Stingray balloon is a flat, self-orientating, over-the-wire balloon with two opposing exit ports that inflates in the subintimal space. Once inflated, the Stingray puncture wire is used to puncture from the subintimal space back into the true lumen of the vessel beyond the blockage. Both devices are manufactured by Boston Scientific.
Yes. The K14 technique has been adopted by CTO operators internationally since publication in Catheterization and Cardiovascular Interventions in 2023. It is referenced in Asia-Pacific CTO Club teaching materials and discussed at major interventional cardiology meetings. It is one of a small number of CTO PCI techniques worldwide to bear the name of its author.
K14 and full ADR technique require operator training in the complete Hybrid CTO Algorithm, access to CrossBoss and Stingray devices, and experience with subintimal navigation. Dr. Arun Kalyanasundaram developed the K14 technique and performs ADR routinely at Promed Hospital, Chennai. He is a co-author of the Asia-Pacific CTO Club CrossBoss/Stingray algorithm published in Catheterization and Cardiovascular Interventions, 2020.
+91 94807 94807
director@ctomd.com
Among India’s most experienced CTO PCI specialists.
Cleveland Clinic-trained.
Asia-Pacific CTO Club India Director.
Dr. Arun Kalyanasundaram is a Chennai-based CTO PCI specialist providing advanced coronary intervention, CTO angioplasty, blocked artery treatment, second opinions, and treatment planning for patients from Mumbai, Delhi, Bangalore, Hyderabad, Pune, Kolkata, Ahmedabad, Chandigarh, Kochi, Visakhapatnam, and throughout India.
Promed Hospital
1/10A East Coast Road, Kottivakkam
Chennai, Tamil Nadu 600041