Peripheral artery disease (PAD) – blockages in the arteries supplying the legs – causes walking pain, poor wound healing, and, when severe, critical limb ischaemia requiring urgent intervention to prevent amputation. Dr. Arun Kalyanasundaram trained in peripheral and structural vascular interventions at the Cleveland Clinic and offers comprehensive endovascular treatment for peripheral arterial disease at Promed Hospital, Chennai.
Peripheral artery disease (PAD) is the narrowing or blockage of the arteries that carry blood to the legs, caused by the same atherosclerotic process that affects the coronary arteries. As plaque builds up, blood flow to the leg muscles and tissues is progressively reduced.
The earliest and most common symptom is intermittent claudication – cramping pain in the calf, thigh, or buttock that comes on with walking and eases with rest. As the disease advances, patients develop rest pain (pain in the foot even when not walking, often worse at night), non-healing wounds and ulcers, and in the most severe cases, tissue loss and gangrene. PAD is also a powerful marker of generalised atherosclerosis – patients with PAD have a substantially elevated risk of heart attack and stroke.
Narrowing of leg arteries causing claudication (walking pain), rest pain, or non-healing ulcers. Treated with balloon angioplasty, stenting, and drug-coated balloon technology.
Complete occlusion of leg arteries, often requiring the same specialist crossing techniques used in coronary CTO PCI – antegrade, retrograde subintimal, and true lumen re-entry.
Severe PAD threatening limb viability – urgent intervention to restore blood flow and prevent amputation. Rest pain, non-healing wounds, or gangrene are warning signs requiring rapid assessment.
Narrowing of arteries supplying the kidneys, causing refractory hypertension and declining kidney function. Catheter-based angioplasty and stenting in carefully selected patients.
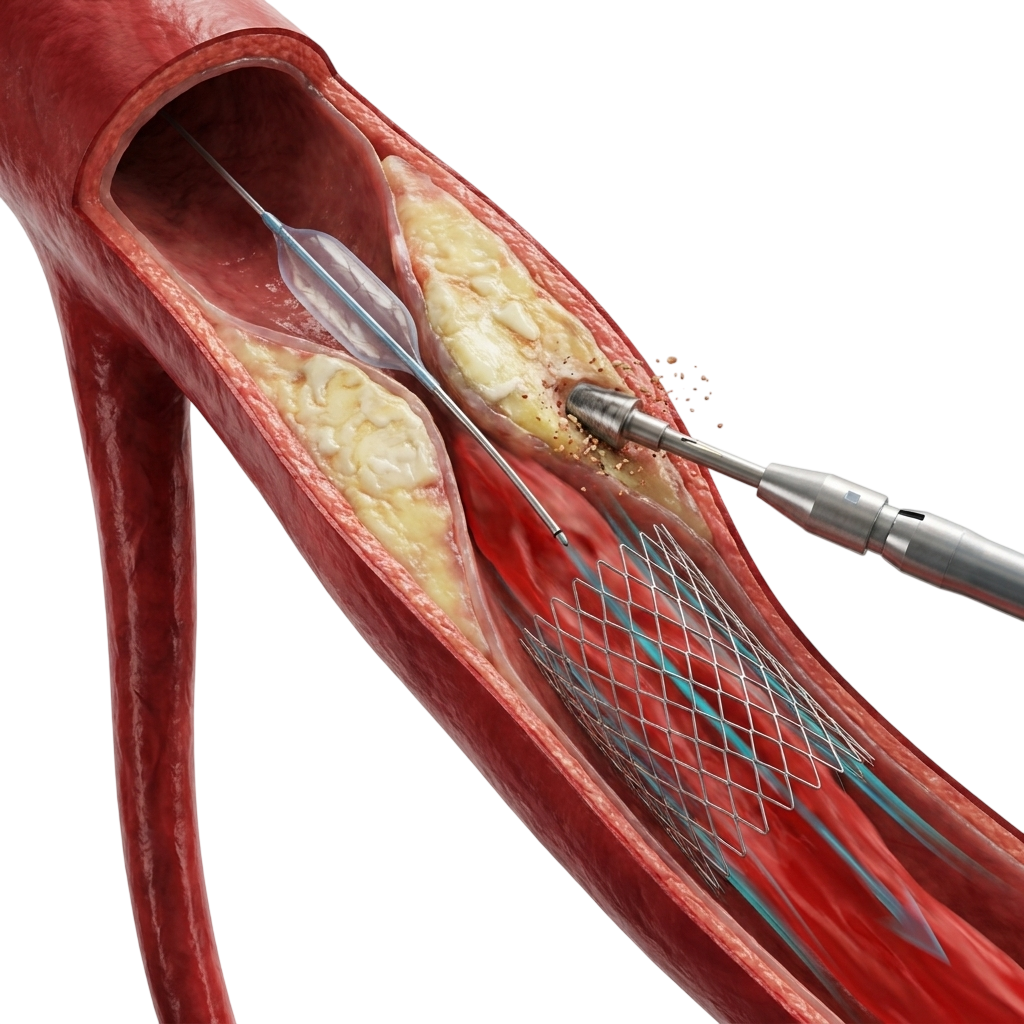
Endovascular treatment for peripheral artery disease uses catheter-based techniques – balloon angioplasty, stenting, and drug-eluting balloon technology – applied to the arteries of the legs, pelvis, and abdomen. Access is achieved through a small puncture in the groin, arm, or even the foot, under local anaesthesia. IVUS assessment provides accurate vessel sizing and confirms stent expansion.
Balloon Angioplasty
First-line treatment for many lesions. A balloon is inflated within the narrowed segment to restore the channel. Suitable for short, focal stenoses.
Drug-Coated Balloons
Reduce restenosis rates in femoral and popliteal segments compared to standard angioplasty – delivering anti-proliferative drug to the vessel wall while leaving no permanent metal behind in segments subject to bending.
Stenting
Self-expanding or balloon-expandable stents for longer lesions, dissections, or recoil after angioplasty. Particularly effective in the iliac arteries of the pelvis.
Imaging-guided Sizing
Intravascular ultrasound provides accurate vessel measurement and confirms stent expansion – the same imaging discipline applied in complex coronary work.
Complete occlusions of the leg arteries often resist standard wires and balloons, requiring the antegrade, retrograde subintimal, and true lumen re-entry techniques that define complex coronary CTO work. An operator who performs high-volume coronary CTO PCI brings directly transferable crossing skills to peripheral recanalisation – wire control, microcatheter support, subintimal navigation, and re-entry.
Dr. Arun Kalyanasundaram’s 2,500+ coronary CTO procedures translate into a distinctive capability for the most challenging peripheral occlusions – the long, calcified, flush occlusions that lower-volume operators often decline.
Peripheral artery disease (PAD) is the narrowing or blockage of arteries supplying the legs, caused by atherosclerosis. The most common early symptom is intermittent claudication - cramping leg or calf pain that comes on with walking and eases with rest. Advanced disease causes rest pain in the foot, coldness or colour change in the limb, and non-healing ulcers. Diagnosis begins with an ankle-brachial index (ABI) measurement and is confirmed with Doppler ultrasound, CT angiography, or invasive angiography.
Yes. Most peripheral artery blockages - including complete blockages (peripheral CTOs) - can be treated with catheter-based endovascular techniques: balloon angioplasty, stenting, and drug-coated balloons. There is no open surgery and no general anaesthesia for most cases. Peripheral CTOs may require the same specialist crossing techniques used in coronary CTO PCI, including subintimal tracking and true lumen re-entry. Endovascular treatment has largely replaced open bypass surgery as first-line therapy for most peripheral disease.
Critical limb ischaemia (CLI) is the most severe form of peripheral artery disease, where blood flow is so reduced that the limb is threatened. It presents as rest pain (pain in the foot even at rest, often worse at night), non-healing wounds, or gangrene. CLI is a limb-threatening emergency requiring urgent intervention to restore blood flow and prevent amputation. Without revascularisation, a significant proportion of CLI patients face major amputation within a year.
A drug-coated balloon (DCB) is an angioplasty balloon coated with an anti-proliferative drug (typically paclitaxel) that is transferred to the artery wall during inflation. It reduces the rate of restenosis — re-narrowing of the treated segment - particularly in the femoral and popliteal arteries of the thigh and knee. DCBs allow effective treatment while leaving no permanent metal stent behind in segments subject to bending and movement, where stents are prone to fracture.
Yes - and this overlap is a significant advantage. A peripheral CTO is a completely blocked leg artery, often requiring the same specialist crossing techniques used in coronary CTO PCI: antegrade wiring, retrograde subintimal tracking, and true lumen re-entry. An operator with high-volume coronary CTO expertise brings directly transferable skills to peripheral CTO recanalisation. Dr. Arun Kalyanasundaram applies his coronary CTO experience to complex peripheral occlusions.
Renal artery stenosis is the narrowing of the arteries supplying the kidneys, usually from atherosclerosis. It can cause refractory hypertension (high blood pressure resistant to multiple medications) and progressive decline in kidney function. In carefully selected patients, catheter-based balloon angioplasty and stenting of the renal artery can improve blood pressure control and stabilise kidney function. Patient selection is critical, as not all renal artery stenosis benefits from intervention.
+91 94807 94807
director@ctomd.com
Among India’s most experienced CTO PCI specialists.
Cleveland Clinic-trained.
Asia-Pacific CTO Club India Director.
Dr. Arun Kalyanasundaram is a Chennai-based CTO PCI specialist providing advanced coronary intervention, CTO angioplasty, blocked artery treatment, second opinions, and treatment planning for patients from Mumbai, Delhi, Bangalore, Hyderabad, Pune, Kolkata, Ahmedabad, Chandigarh, Kochi, Visakhapatnam, and throughout India.
Promed Hospital
1/10A East Coast Road, Kottivakkam
Chennai, Tamil Nadu 600041