Severely calcified coronary arteries cannot be treated with standard angioplasty balloons and stents alone. Calcium prevents stent expansion – leading to underexpanded stents, in-stent restenosis, and stent thrombosis.Dr. Arun Kalyanasundaram uses imaging-guided rotational, orbital, and laser atherectomy and intravascular lithotripsy to prepare calcified lesions before stenting – achieving fully expanded, durable stents that balloon-only preparation cannot reliably produce.
If you have been told your artery “cannot be stented” due to calcium, or if a previously placed stent did not expand properly, imaging-guided calcified lesion preparation may help clarify your options. Get a Second Opinion →
Calcium deposition in coronary arteries is a consequence of chronic atherosclerosis. Over years, lipid-rich plaques become fibrotic and eventually calcified as the body deposits hydroxyapatite crystals within the arterial wall. Superficial calcium – located in the inner layers – is amenable to modification with rotational atherectomy. Deep circumferential calcium – encircling the full thickness of the vessel wall – creates a rigid sleeve that stents cannot penetrate or deform. This is the most clinically significant form.
When a stent is deployed in a heavily calcified artery without adequate lesion preparation, the stent does not fully expand – it remains constricted at the calcium deposits, creating zones of severe underexpansion. Underexpanded stents are associated with dramatically increased rates of in-stent restenosis and stent thrombosis. This is one of the most preventable causes of PCI failure, and it is prevented by calcium modification before stenting.
Angiography dramatically underestimates the extent of coronary calcification. A lesion that appears moderately calcified on fluoroscopy may have severe circumferential calcium on IVUS. This discrepancy has significant implications for procedural planning. IVUS allows the operator to measure:
These technologies are available in Dr. Arun’s cath lab. The choice between them – or their combination (“Rotatripsy”) – is driven by IVUS assessment of calcium depth and pattern, not by which device happens to be on the shelf.
A diamond-coated burr rotating at 140,000–180,000 RPM is advanced over a dedicated guidewire and tracks through the calcified segment. The high-speed rotation ablates superficial calcium by a differential cutting mechanism – the burr cuts hard calcium but deflects around soft plaque tissue. This modifies the lesion to allow passage of a standard balloon and adequate stent expansion. Rotablation generates microparticles smaller than red blood cells, cleared by the reticuloendothelial system.
RPM Burr Speed
Clinical Evidence
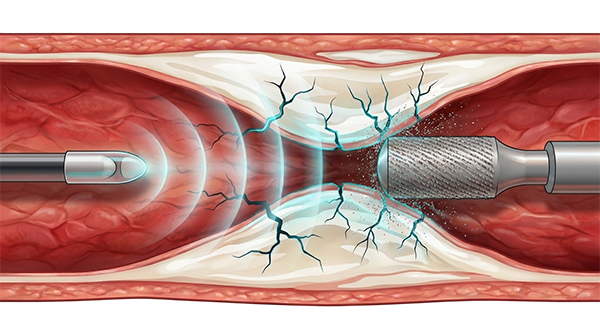
IVL uses sonic pressure waves – analogous to extracorporeal lithotripsy for kidney stones – to fracture calcified plaque from within the coronary artery. A dedicated balloon catheter containing lithotripsy emitters is positioned at the calcified segment and inflated at low pressure, activating the emitters to generate localised sonic pulses. These pulses propagate through tissue and fracture calcium at depth without requiring direct contact with the calcium surface. Because IVL works at depth, it is effective against deep circumferential calcium that rotational atherectomy cannot reach.
Balloon Pressure
Calcium Reach
Deep, circumferential calcium resistant to rotablation. Long calcified segments. Cases where rotablation has been attempted but insufficient calcium modification achieved. Calcified lesions with stent underexpansion from prior procedures – IVL within the stent fractures constraining calcium.
An orbitally rotating, diamond-coated crown sands away calcified plaque as it moves eccentrically through the vessel, modifying calcium on both forward and backward passes. Useful for diffuse superficial and moderately deep calcium.
Excimer Laser Coronary Atherectomy uses pulsed ultraviolet energy to ablate plaque and thrombus. Useful for uncrossable or undilatable lesions, under-expanded stents, and lesions with associated thrombus.
A stent placed in a heavily calcified artery without adequate lesion preparation typically does not fully expand - constrained by the rigid calcium at one or more points. Underexpanded stents have markedly higher rates of in-stent restenosis (typically at 6–12 months) and stent thrombosis (which can cause a heart attack). This is preventable with IVUS assessment and appropriate lesion preparation with rotablation or IVL.
Yes. IVL can be used inside a previously deployed stent to fracture the calcium causing underexpansion, allowing the stent to be further expanded with a high-pressure balloon. This approach - sometimes called "lithotripsy for undilatable stents" - is particularly useful when a stent has already been placed and cannot be fully expanded despite high-pressure balloon inflation. Dr. Arun Kalyanasundaram performs this type of redo intervention routinely.
Rotational atherectomy is a well-established technique with over 30 years of use in interventional cardiology. In experienced hands, it has an acceptable safety profile. The main risks include coronary artery spasm (managed with vasodilator medications pre-procedure), the no-reflow phenomenon (reduced blood flow after burr passage, typically transient), and perforation (rare with appropriate burr sizing). These risks are known, anticipated, and managed systematically.
Rotablation (rotational atherectomy) uses a diamond-coated burr spinning at 140,000–180,000 RPM to ablate superficial calcium by differential cutting. IVL (intravascular lithotripsy) uses sonic pressure waves to fracture deep calcium at depth without direct contact. Rotablation is best for superficial nodular calcium that prevents balloon crossing; IVL is best for deep circumferential calcium and for fracturing calcium inside underexpanded stents. The choice is guided by IVUS assessment of calcium depth and pattern.
Angiography dramatically underestimates calcification. A lesion that appears moderately calcified on fluoroscopy may have severe circumferential calcium on intravascular ultrasound (IVUS). Definitive assessment requires IVUS or OCT imaging, which measures the arc of calcium in degrees, its depth, and its length. If you have been told your artery cannot be stented due to calcium, an IVUS-guided second opinion can determine whether modern calcium modification with rotablation or IVL makes stenting feasible.
Recovery after calcified lesion intervention is similar to standard angioplasty. Most patients stay in hospital for one to two nights. Dual antiplatelet therapy is prescribed for 12 months after drug-eluting stent placement. The calcium modification itself does not extend recovery time - it is performed during the same procedure as stenting. Follow-up at 4-6 weeks with functional assessment at 3-6 months is standard.
+91 94807 94807
director@ctomd.com
Among India’s most experienced CTO PCI specialists.
Cleveland Clinic-trained.
Asia-Pacific CTO Club India Director.
Dr. Arun Kalyanasundaram is a Chennai-based CTO PCI specialist providing advanced coronary intervention, CTO angioplasty, blocked artery treatment, second opinions, and treatment planning for patients from Mumbai, Delhi, Bangalore, Hyderabad, Pune, Kolkata, Ahmedabad, Chandigarh, Kochi, Visakhapatnam, and throughout India.
Promed Hospital
1/10A East Coast Road, Kottivakkam
Chennai, Tamil Nadu 600041